
The regulations every NHS estates team works to.
NHS premises are non-domestic and high-risk by default, with sleeping accommodation, vulnerable occupants, and complex evacuation strategies. The Fire Safety Order applies, but Firecode is the framework Trusts actually work to. Here is what sits behind every estates compliance review.
Fire Safety Order 2005
Article 8 imposes a duty on the Responsible Person to take general fire precautions across all NHS premises. The Chief Executive of the Trust is the legally accountable RP, with day-to-day delegation to the Estates and Facilities Director.
HTM 05-02: Firecode design
Health Technical Memorandum on fire safety in the design and management of healthcare premises. Sets the structural fire safety, compartmentation, and door specification standards every Trust capital and refurbishment project follows.
HTM 05-03: Firecode operational
The operational provisions overlay covering inspection regimes, staff training, premises management, and evacuation procedures. The day-to-day reference framework every NHS estates team works against, parts A through H.
BS 9999:2017
Code of practice for fire safety design and management of buildings. Applied across the NHS estate where HTM 05-02 cross-references or defers to it, particularly on door performance, hardware specification, and inspection protocols.
Building Safety Act 2022
Higher-risk buildings above eighteen metres or seven storeys carry the Accountable Person duty and Building Safety Regulator registration. A meaningful slice of the NHS hospital estate qualifies, particularly tower-block-era acute hospitals.
CQC Fundamental Standards
Regulation 12 (safe care and treatment) and Regulation 15 (premises and equipment) are read in light of fire safety compliance. CQC inspectors expect documented fire door evidence on demand, and an inspection gap is a Regulation 15 risk.
Built around how NHS estates actually operate.
DoorTRACE configures around the NHS estates reality: Firecode language, clinical access windows, PFI split responsibility, and a CQC inspector who can arrive at the door tomorrow.
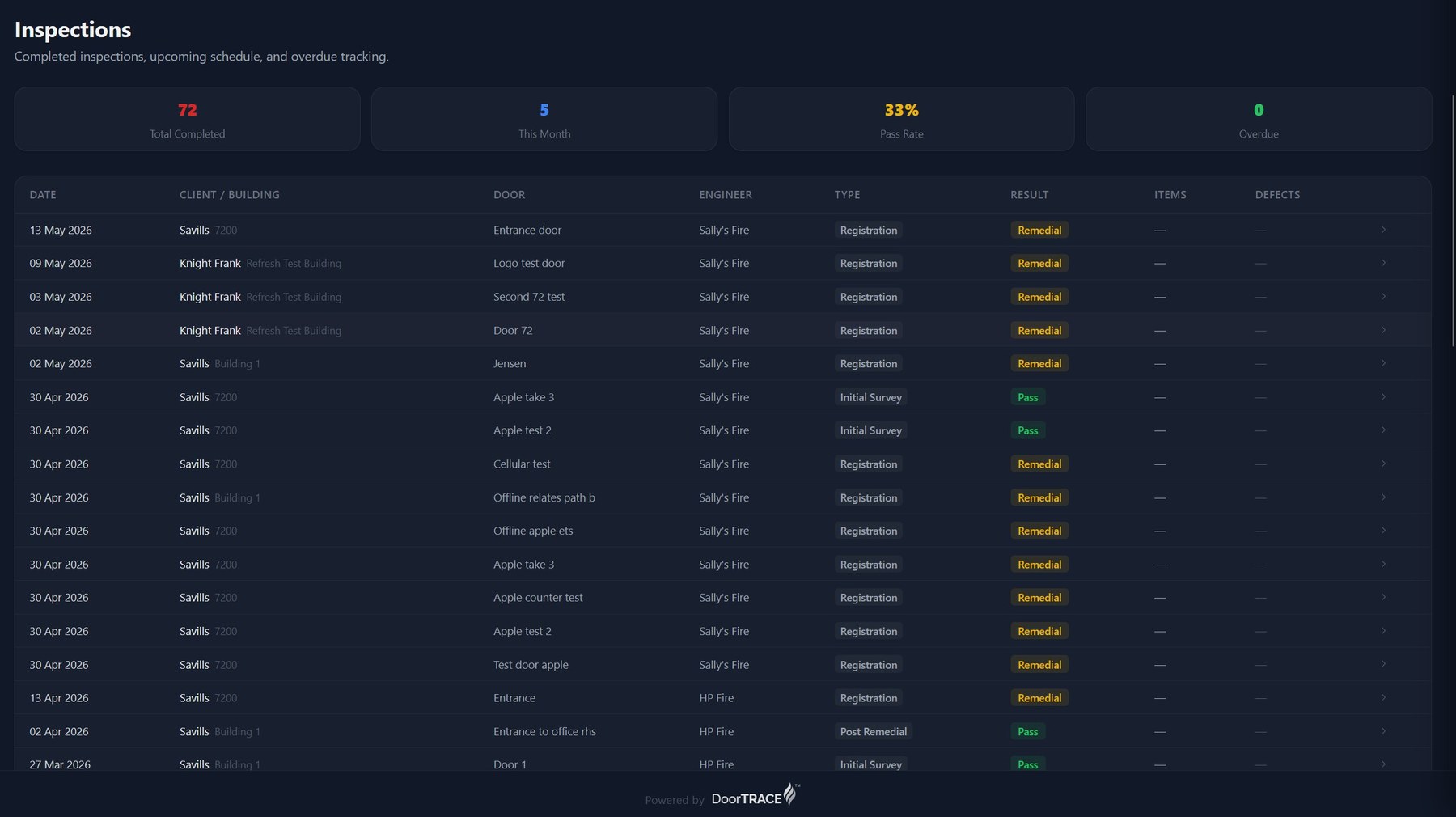
HTM 05-03 inspection cycles, tracked at site level.
Inspection cadence configured against HTM 05-03 operational provisions, by department and by clinical risk. Theatre suites, critical care, and infection-control zones get the appropriate inspection windows. The Estates Director sees real-time cycle status across every site, every wing, every clinical area, every fire door.
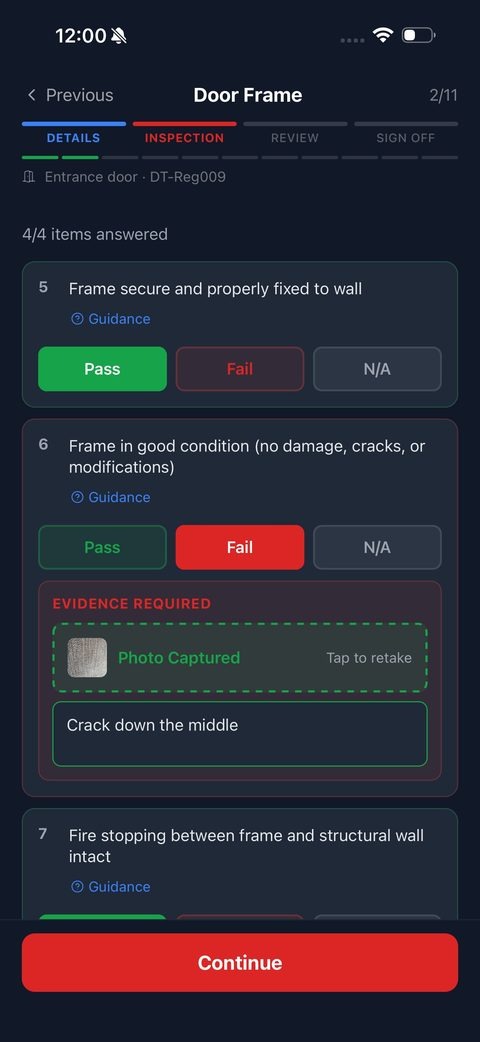
An engineer app that respects clinical reality.
Engineers see clinical-area access notes and infection control protocols before they arrive on the ward. They can defer an inspection for active patient care, photograph it, log the deferral with reason, and re-book through the ward team. The audit trail shows the inspection was attempted, deferred for clinical reasons, and completed: the only defensible evidence chain in a CQC review.
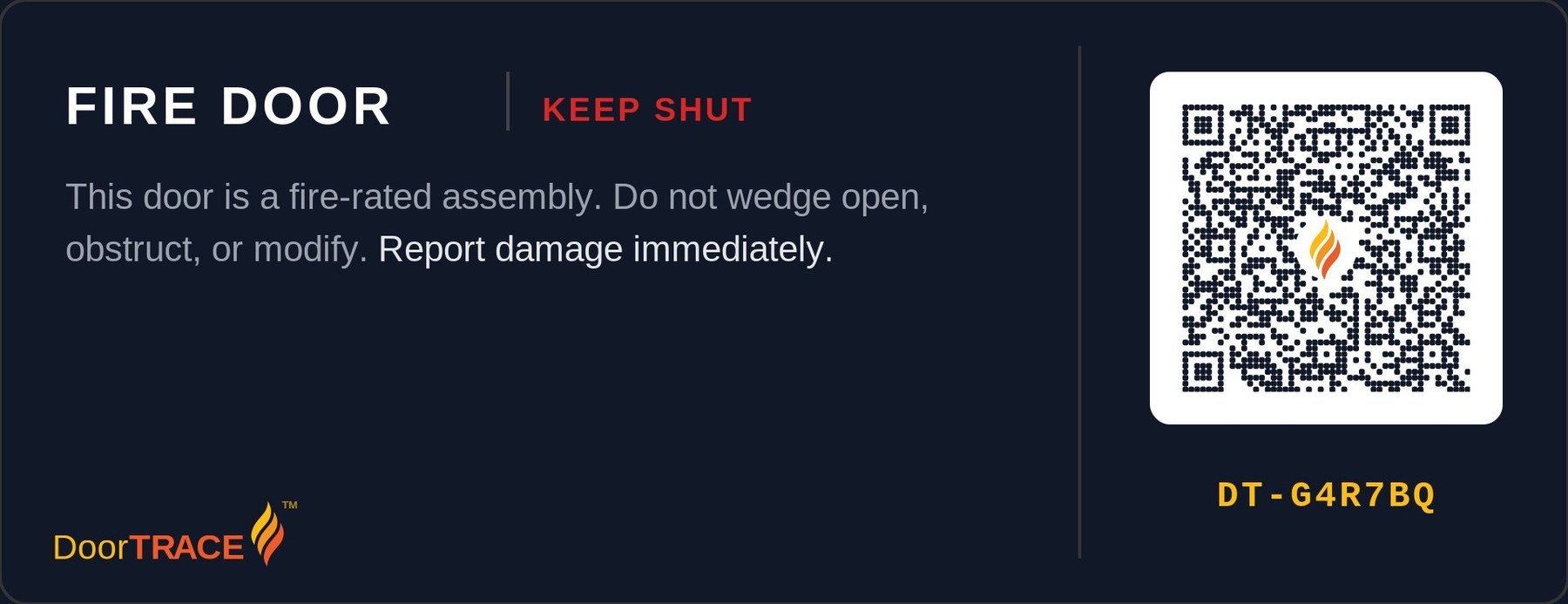
A plaque every inspector can scan.
Every fire door carries a QR plaque. CQC inspectors, fire authority officers, Trust auditors, and PFI consortium engineers can verify the door from their own phone in seconds. Plaques survive cleaning regimes, decontamination protocols, and corridor traffic loads. They also link the right inspection record to the right physical door, every time.
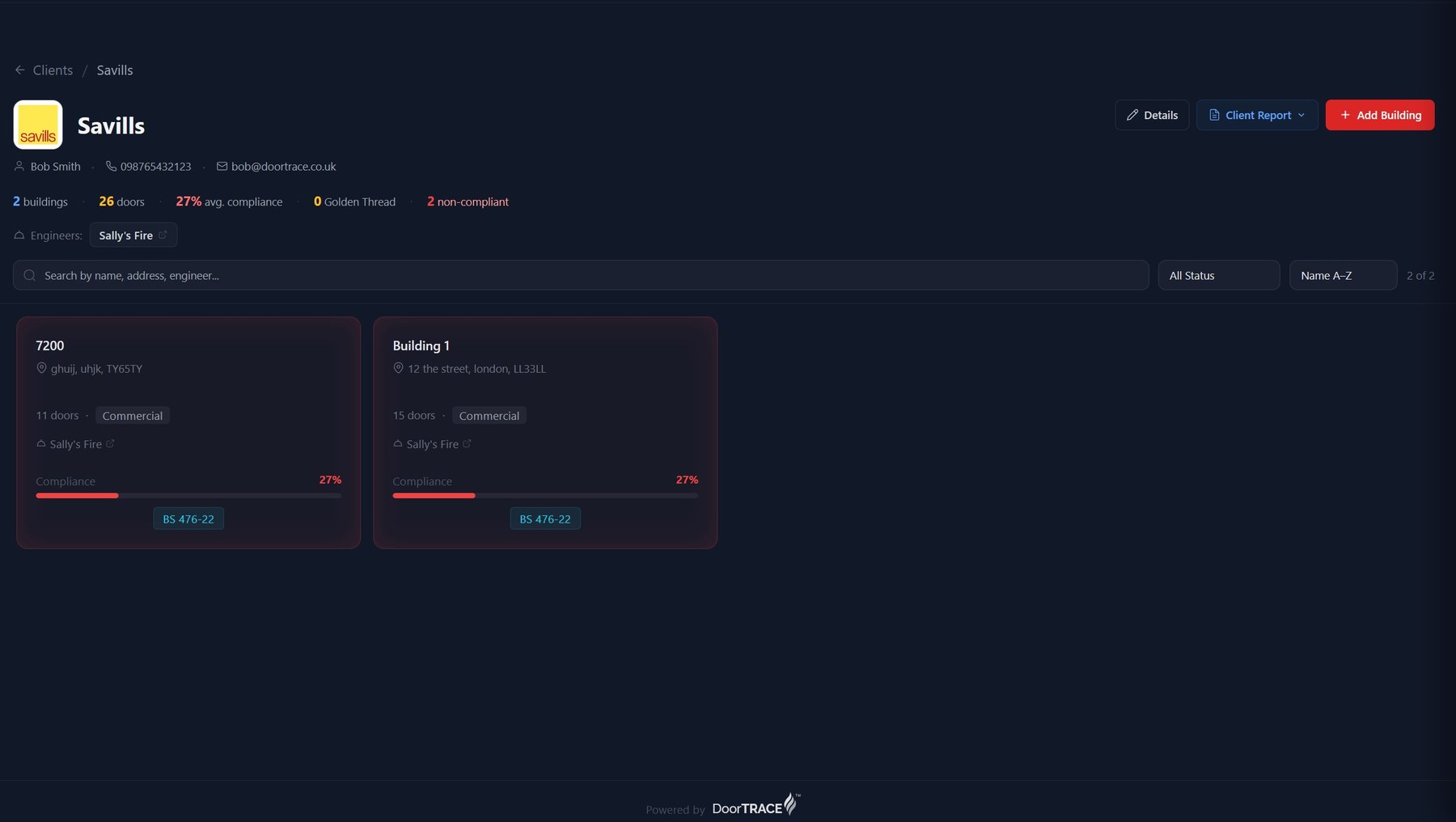
Every site, every wing, one Firecode record.
Site-level compliance status, by building, by department, by clinical risk tier. PFI buildings clearly marked with the responsibility split. Drill into any door for the full history: every inspection, every defect, every photo, every remedial work order. Export a CQC inspection evidence pack in two clicks, a Trust Board compliance summary in five.
The NHS estate, in fire door terms.
A week in the life of an NHS Trust estates director.
It is 08:00 on a Monday. The Estates and Facilities Director of a 900-bed NHS acute Trust opens DoorTRACE before the executive team meeting at nine.
The dashboard shows two wards amber: the cardiology corridor has an inspection due in seven days, and the rehab unit has an outstanding closer defect from the last visit. He assigns the in-house engineer to cardiology and routes the closer defect to the PFI consortium's CAFM system through the integration. Both updates land before the nine-o'clock executive meeting.
Engineer in the cardiology corridor logs a self-closer fault on a ward-to-family-room fire door. The fault sits inside the PFI consortium's hard FM scope, so the defect routes automatically to Sodexo's work order system with a P2 response time. The Trust's legal evidence trail stays intact in DoorTRACE.
A CQC inspector arrives unannounced at the rehab unit. The estates lead pulls the building's full fire door evidence on a tablet: every door, every inspection, every defect with resolution dates, every remedial photo. The inspector asks about one specific corridor door near the day room; the full history surfaces in five clicks. The visit closes without compliance findings.
The Trust Executive board pack auto-generates: portfolio compliance percentage by site, top five defects by clinical area, CQC visit summary, BSR HRB status for the tower-block hospital, and the open PFI defect list. The Estates Director shares it with the Chief Executive ahead of the Monday board meeting.